Webinar II - "Frauen mit Diabetes in den Wechseljahren"
25.06.2026; 18:00 - 19:30 Uhr, Online per Zoom
Referentin: Martina Rothenbühler, Bern
Die hormonellen Veränderungen in der Peri-Menopause und Menopause stellen für Frauen mit Typ-1-Diabetes eine oft unterschätzte Herausforderung dar. Der Rückgang des Östrogens führt zu verminderter Insulinsensitivität und erhöhter glykämischer Variabilität, während hormonelle Schwankungen unvorhersehbare Blutzuckerverläufe hervorrufen können. Zusätzlich steigt das kardiovaskuläre Risiko, da sowohl Menopause als auch T1D ungünstige Effekte auf Stoffwechsel und Gefäßgesundheit haben. Aktuelle Diabetes-Technologien sind auf diese Lebensphase bislang nur unzureichend angepasst.
In dem Webinar wollen wir auf diese Aspekte eingehen und freuen uns auf eine rege Teilnahme.
Der Link für die Teilnahme wird den Mitgliedern des Vereins rechtzeitig vor dem Webinar mitgeteilt.
Interessenten bitte an kontakt@diabetes-psychologie.de wenden
Fortbildungspunkte werden bei der PTK beantragt.
Die Teilnahme ist kostenfrei.
Webinar III - Thema noch nicht festgelegt
Termin: im 3. Quartal, wird noch bekannt gegeben
Fortbildungspunkte werden bei der PTK beantragt.
Die Teilnahme ist kostenfrei.
Jahrestagung Diabetes und Psychologie e. V.
Arbeitsgemeinschaft "Diabetes und Psychologie" DDG
Programm wird noch festgelegt
Freitag, 25.09.2026 - Sonntag, 27.09.2026
Online per Zoom, kostenfrei
Anmeldung
Eine Anmeldung zur Jahrestagung ist zwingend erforderlich.
Bitte vor der Tagung per E-Mail unter kontakt@diabetes-psychologie.de
unter Angabe des Berufes, Adresse und E-Mailadresse anmelden. Die
einzelnen Zugangslinks werden einige Tage vor der Jahrestagung an die
angegebene Mailadresse zugesandt.
Webinar IV - "minDBe: Vorstellung eines Manuals für Menschen mit Diabetes und erhöhten diabetesbezogenen Belastungen"
29.10.2026; 18:00 - 19:30 Uhr, Online per Zoom
Referentin: PD Dr. Hanna Kampling, Gießen
Kurzbeschreibung folgt.
Der Link für die Teilnahme wird den Mitgliedern des Vereins rechtzeitig vor dem Webinar mitgeteilt.
Interessenten bitte an kontakt@diabetes-psychologie.de wenden
Fortbildungspunkte werden bei der PTK beantragt.
Die Teilnahme ist kostenfrei.
Webinar I - "Stigma Diabetes?"
05.03.2026; 18:00 - 19:30 Uhr, Online per Zoom
Referent: Prof. Dr. Bernhard Kulzer, Bad Mergentheim
Menschen mit Diabetes erleben
häufig Stigmatisierungen.
In dem Webinar sollen die
verschiedenen Ebenen der Stigmatisierung aufgezeigt sowie ein Überblick über
den Stand der Literatur zum Thema „Stigmatisierung bei Diabetes“ gegeben
werden. Zudem werden die Ergebnisse
einer aktuellen deutschen Studie bei Menschen mit Diabetes vorgestellt und
psychotherapeutische Strategien zum Umgang mit Diabetesstigma diskutiert.
Der Link für die Teilnahme wird den Mitgliedern des Vereins rechtzeitig vor dem Webinar mitgeteilt.
Interessenten bitte an kontakt@diabetes-psychologie.de wenden.
Das Webinar wurde mit 3 Fortbildungspunkten der Landespsychotherapeutenkammer Baden-Württemberg zertifiziert.
Die Teilnahme ist kostenfrei.
Termine 2025
Webinar IV - "Determinanten psychischer Störungen bei Diabetes"
06.11.2025; 18:00 - 19:30 Uhr, Online per Zoom
Referent: Dr. Andreas Schmitt, Bad Mergentheim
Der Zoom-Link für die Teilnahme wird den Mitgliedern des Vereins rechtzeitig vor dem Webinar mitgeteilt.
Interessenten bitte an kontakt@diabetes-psychologie.de wenden.
Das Webinar wurde mit 3 Fortbildungspunkten der Landespsychotherapeutenkammer Baden-Württemberg zertifiziert.
Für den Erhalt eines Zertifikates bitte im Chatverlauf den Vor- und Zunamen eintragen, zusätzlich nach dem Webinar eine E-Mail an kontakt@diabetes-psychologie und Name/Straße/PLZ/Ort mitteilen.
Kickoff-Meeting für
"Früh vernetzt - Nachwuchs Psychodiabetologie"
09.10.2025; 18:00 - 19:00 Uhr, Online per Zoom
Laura Klinker und Theresa Mohr
Wir möchten junge Wissenschaftler und Praktiker speziell fördern und freuen uns sehr, dass Laura Klinker (Bad Mergentheim) und Theresa Mohr (Amsterdam) eine Arbeitsgruppe zum Thema für "Früh vernetzt - Nachwuchs Psychodiabetologie" gründen möchten.
Das Treffen wendet sich an alle jungen Kolleginnen/Kollegen, die an dieser AG mitmachen möchten.
Auch hier gilt: Vorab eine kurze E-Mail an kontakt@diabetes-psychologie.de und schon kommt der Zoom-Link.
"Diabetes - Leben mit Unsicherheiten"
Jahrestagung Diabetes und Psychologie e. V.
Arbeitsgemeinschaft "Diabetes und Psychologie" DDG
Freitag, 26.09.2025 - Sonntag, 28.09.2025
Online per Zoom, kostenfrei
Anmeldung
Eine Anmeldung zur Jahrestagung ist zwingend erforderlich.
Bitte vor der Tagung per E-Mail unter kontakt@diabetes-psychologie.de unter Angabe des Berufes, Adresse und E-Mailadresse anmelden. Die einzelnen Zugangslinks werden einige Tage vor der Jahrestagung an die angegebene Mailadresse zugesandt.
Das Leben mit Diabetes ist geprägt durch Risiken, Unsicherheiten
und mannigfache Heraus-forderungen, die es zu meistern gilt. In unserer Tagung
versuchen wir einen weiten Bogen zu spannen: Von den Unsicherheiten unserer
Gegenwart mit dem oft entfremdeten Selbst und den Veränderungen durch die
Digitalisierung, künstliche Intelligenz, die zunehmend das Leben von Menschen
mit Diabetes und uns Behandler bestimmt - der Ursache von Unsicherheiten bei
Diabetes, die häufig durch Mikro- und Makrotraumen in der Lebensgeschichte bedingt
sind - bis hin zu Forschungsergebnissen und therapeutischen Konzepten bei Unsicherheiten,
Risiken im Leben mit Diabetes.
Wir hoffen, dass diese Themen
auch für Sie spannend sind und freuen uns auf eine inspirierende,
diskussionsfreudige und ergebnisreiche Tagung. Nehmen Sie teil, machen Sie mit!
PD Dr. Hanna Kampling * Prof. Dr. Bernd Kulzer * Dr. Andreas
Schmitt
Freitag, 26.09.2025
15.30 – 17.30 Mitgliederversammlung (nur für
Mitglieder)
Vorsitz: Prof.
Dr. Bernd Kulzer, Bad Mergentheim
Freitag 26.09.2025 Jahrestagung
Vorsitz: PD Dr. Hanna Kampling (Gießen)
18:00 - 19:30 Uhr Das parasozial
entfremdete Selbst
Dr.
Johanna Degen (Flensburg)
Samstag, 27.09.2025
Ambiguität, Risiken, Zukunftsoptionen
Vorsitz: Dr. Marion Hagemann-Goebel (Hamburg)
09:00 -
09:45 Uhr Umgang
mit Risiken des Diabetes
Prof. Dr. Bernd Kulzer (Bad Mergentheim)
09:45 -
10:30 Uhr Digitalisierung, KI und
Psychodiabetologie
Prof. Dr. Harald
Baumeister (Ulm)
10:30
-10:45 Uhr Pause
Traumafolgestörungen
Vorsitz: Uwe Schönrade (Köln)
10:45 - 11:30 Uhr Diabetes und Trauma
Prof. Dr. Johanns Kruse (Gießen)
11:15 - 12:15 Uhr Vom Trauma zu gezielten Therapie
PD Dr. Hanna Kampling (Gießen)
12:15 – 13:15 Uhr Mittagspause
Unsicherheiten im
Leben mit Diabetes
Vorsitz: Dr. Ulrike Löw
(Frankfurt)
13:15 – 13:45 Uhr Diabetesbezogene Sorgen und Ängste
Dr. Andreas Schmitt (Bad Mergentheim)
13:45 – 14:15 Uhr Subjektive Bewertungen und Belastungen
durch Glukoseschwankungen
Prof. Dr. Norbert Hermanns (Bad
Mergentheim)
14:15 –
14:45 Uhr MyDiaMate: Mehr Sicherheit im
Umgang mit Herausforderungen des Diabetes mit einer webbasierten Selbstlern-App
zur psychischen Gesundheit
Theresa Mohr (Amsterdam)
14:45 – 15:15 Uhr Verläufe von Diabetes-Belastungen (EMA)
Kristina
Katzenberger (Würzburg)
15:15 – 15:30 Uhr Zusammenfassung
Sonntag, 28.09.2024
Workshops
Vorsitz: Eva Küstner (Gau-Bischofsheim)
09:00 -
10:00 Uhr Psychologische Mechanismen
in digitaler Ratsuche und AI-gesteuerter Beratung
Dr. Johanna Degen
(Flensburg)
10:00 –
11:00 Uhr Chancen und Limitationen von
webbasierten Selbstlern-Apps zur psychischen Gesundheit
Theresa Mohr
(Amsterdam), Prof. Dr. Norbert Hermanns (Bad Mergentheim)
Die Tagung erfolgt über die
Plattform Zoom und ist kostenfrei. Der Link für die Mitgliederversammlung wird
den Mitgliedern mit der Einladung zugesandt.
Fortbildungspunkte wurden bei
der Psychotherapeutenkammer Baden-Württemberg und dem Verband der Beratungs-
und Schulungsberufe in Deutschland (VDBD) beantragt, Fortbildungspunkte siehe Agenda.
Für den Nachweis der Fortbildungspunkte ist
wichtig:
• Am
26.09.2025: Einwahl zwingend zwischen 18.00 – 18.30 mit Klarnamen sowie zusätzlich Rückmeldung per E-Mail an kontakt@diabetes-psychologie.de
• Am
27.09.2025: Einwahl
zwingend zwischen 09.00 – 09.30 und 14.00 -14.30 mit Klarnamen sowie zusätzlich Rückmeldung per E-Mail an kontakt-diabetes-psychologie.de
• Am
28.09.2025: Einwahl
entsprechend der Teilnahme an den Workshops in den ersten 30 Minuten jedes
Workshops mit Klarnamen sowie zusätzlich per E-Mail an kontakt@diabetes-psychologie.de
Webinar III - "Progredienzangst in der ambulanten Gruppentherapie“
04.09.2025; 18:00
-19:30 Uhr, Online per Zoom
Referentin: Dr.
Sabine Waadt, München
Der Zoom-Link für die Teilnahme wird den Mitgliedern des Vereins rechtzeitig vor dem Webinar mitgeteilt.
Interessenten bitte an kontakt@diabetes-psychologie.de wenden
Progredienzangst ist für MmD eine der wichtigsten und häufigsten Belastungen. Anders als bei anderen chronischen Erkrankungen, z.B. Ca oder MA tritt sie meist weniger in direkter Äußerung in Erscheinung sondern ist als Hintergrundstimmung oder intrusiver Affekt in sehr unterschiedlichen Problemlagen wirksam, wie z.B. resignativer Vermeidung der Behandlung, Vermeidung von Autofahren, Ärger bei Terminirritationen, Störungen der Behandlungskonstanz oder übermäßig häufigen Eingriffen in die Pumpen-Allgorhythmen.Muss Progredienzangst daher bereits in der Einzelpsychotherapie in unterschiedlichsten Themen erkannt werden, bestehen für die ambulante PT Gruppenbehandlung zusätzliche Herausforderungen. So können z.B. gute HbA1c-Werte für Teilnehmende mit erhöhter Blutzuckerlage eine extreme Angst- und Scham-Exposition bedeuten, die eine PA Benennung verhindern und sogar zu Therapieabbruch führen können. Die relativierende Reflexion über Kontrollexzesse wiederum kann Ärger und Abwehr gegenüber vermeintlicher Bedrohung der Gesundheitsvorsorge auslösen. PA erfordert daher in Gruppen nicht nur ein inhaltliche Auseinandersetzung mit Krankheitsängsten, sondern auch mit Mentalisierungsprozessen und der Toleranz unterschiedlicher Selbstbilder.Dargestellt werden die besonderen Bedingungen einer ambulanten D.m. Gruppenbehandlung die PA-Behandlung integrieren möchte sowie einmalige und wiederholende Strategien und Materialien.
Das Webinar wurde mit 3 Fortbildungspunkten der Psychotherapeutenkammer Baden-Württemberg bewertet.
Für
den Erhalt eines Zertifikates bitte im Chatverlauf den Vor- und Zunamen
eintragen, zusätzlich nach dem Webinar eine E-Mail an kontakt@diabetes-psychologie.de und Name/Straße/PLZ/Ort mitteilen.
Die Teilnahme ist kostenfrei.
Webinar II - Diagnose "Diabetes" bei
Kindern, Jugendlichen und deren Eltern - erste psychologische
Unterstützung mit prägender Bedeutung
12.06.2025; 18:00 -19:30 Uhr,Online per Zoom
Referent: Dr. Berthold Maier, Bad Mergentheim
Erfahren Kinder, Jugendliche und deren Eltern von der Diagnose
eines Diabetes, reagieren Familien häufig hoch belastet und
verunsichert. Vielfach beschreiben Eltern das Gefühl, "den Boden unter
den Füßen zu verlieren" und benötigen Zeit, bis sie die Diagnose als
Tatsache anerkennen und realisieren können. Gleichzeitig sorgen sich die
Eltern um das Wohlergehen ihres Kindes, manche äußern Schuldgefühle,
gleichzeitig müssen Therapien und Versorgung geplant und organisiert
werden - und der Alltag muss irgendwie weitergehen. Kinder, Jugendliche
und ihre Eltern müssen sich in vielerlei Hinsicht auf neue Gegebenheiten
einstellen. Komplexe Therapieanforderungen müssen nicht nur ins
Familienleben, sondern auch in Abläufe im Kindergarten, in der Schule,
bei der Ausbildung, bei Sport und in der Freizeit integriert werden.
Vielfach beschreiben sich alle Familienmitglieder in den ersten Wochen
und Monaten hoch angespannt, vor allem die Mütter, die häufig die
Hauptverantwortung für die Diabetesbehandlung übernehmen. Gerade in
dieser belastenden Phase nach der Diagnose brauchen Familien gezielte
psychologische und sozialrechtliche Unterstützung.
Das Webinar ist auch geöffnet für Familien, die Gelegenheit haben, ihre
individuellen Fragen direkt Psychologinnen und Psychotherapeuten zu
stellen. Neben dem fachlichen Austausch unter Fachleuten sollen Familien
auch einen Zeitkorridor nutzen können, um direkte Antworten zu
erhalten. Die Veranstaltung erfolgt in Kooperation mit dem Deutschen
Diabetiker Bund, der dieses Webinar auch seinen sozialen Kanälen
kommunizieren wird.
Wir freuen uns auf Ihre Teilnahme!
Webinar I - "Resilienz bei bestehenden Folgeerkrankungen"
13.03.2025; 18:00
– 19:30 Uhr, Online per Zoom
Referent: Dr. Berthold Maier, Bad Mergentheim
Die Diagnose einer Folgeerkrankung, aber auch das Erleben der
Unumkehrbarkeit sowie des Fortschreitens der Beschwerden zählen zu den
stärksten Stressoren für Menschen mit Diabetes. Wie neuere Daten zeigen,
haben Menschen mit Diabetes und Folgeerkrankungen ein bis zu 3-fach
erhöhtes Risiko für die Entstehung einer psychiatrischen Erkrankung (z.
B. Angststörung, Depression), verglichen mit Menschen ohne Diabetes.
Umgekehrt gelingt es einigen Menschen mit diabetischen
Folgeerkrankungen, trotz der kontinuierlichen Belastungen psychisch
stabil zu bleiben. Das zeigen sowohl die Daten als Erfahrungen aus der
klinischen Praxis.
Welches sind die spezifischen Mechanismen und Faktoren für Resilienz bei
bestehenden Folgeerkrankungen?
Welche Interventionen könnten helfen, die Resilienz bei dieser großen
Personengruppe zu stärken und der Entwicklung psychischer Erkrankungen
vorzubeugen?
Ziel des Webinars ist, nach einem kurzen inhaltlichen Impuls
Resilienzfaktoren im Austausch zu ermitteln und resilienzstärkende
Hilfen bei bestehenden Folgeerkrankungen abzuleiten.
Therapie der Adipositas, Essstörungen bei Diabetes: Neue Perspektiven
Jahrestagung der AG Diabetes und Psychologie, DDG
"Diabetes und Psychologie e.V."
27.09.2024 - 29.09.2024 online per Zoom
Eine vorherige Anmeldung ist nicht nötig. Am Veranstaltungstag können Sie einfach über den jeweiligen Zoom-Link teilnehmen. Jeder Tag hat einen eigenen Zugangslink für Zoom.
Freitag, 27.09.2024
15:30 – 17:30 Uhr Mitgliederversammlung (nur für
Mitglieder)
Zoom-Link: Per mail an alle Mitglieder
Vorsitz: Prof.
Dr. Bernd Kulzer, Bad Mergentheim
18:00 – 19:30 Uhr Soziokulturelle
Aspekte von Essstörungen, Adipositas
Workshops
Vorsitz: Dr.
Berthold Maier, Bad Mergentheim
09:00 –
10:00 Uhr Adipositas im Fokus der Psychotherapie
Dr. Marion
Hagemann-Goebel, Hamburg; Dr. Ulrike Löw, Frankfurt
10:00 –
11:00 Uhr Screening, Diagnostik und
Therapie von Binge Eating Disorders
Laura Klinker,
Bad Mergentheim
11:00 – 12:00 Uhr Digitale Anwendungen bei Essstörungen
Dr. Jenny Grammes, Mainz
Die Tagung
erfolgt über die Plattform Zoom und ist kostenfrei. Der Link für die
Mitgliederversammlung wird den Mitgliedern mit der Einladung zugesandt.
Fortbildungspunkte:
Psychologen, Psychotherapeuten: Freitag, 27.09.24: 2 Punkte; Samstag, 28.09.24 Vormittag: 5
Punkte; Samstag, 28.09.2024 Nachmittag: 2 Punkte Sonntag, 29.09.24 2 Punkte je
Workshop. Bei vollständiger Teilnahme: 15 Fortbildungspunkte.
VDBD: Freitag,
27.09.24: 2 Punkte; Samstag, 28.09.24: 7 Punkte; Sonntag, 29.09.24: 1 Punkte je
Workshop. Bei vollständiger Teilnahme: 12 Fortbildungspunkte
Für den Nachweis der Fortbildungspunkte ist
wichtig:
• Am
27.09.2024: Einwahl zwingend zwischen 18.00 – 18.30 mit Namen
• Am
28.09.2024: Einwahl
zwingend zwischen 09.00 – 09.30 und 14.00 -14.30 mit Namen
• Am
29.09.2024: Einwahl
entsprechend der Teilnahme an den Workshops in den ersten 30 Minuten jedes
Workshops mit Namen
Für den Erhalt eines Zertifikates bitte eine E-Mail an Frau Kalwach kalwach@fidam.de mit Angaben des Vor- und Zunamen, Beruf, Straße, PLZ und Wohnort senden.
Die
psychologische Therapie von Menschen mit Diabetes ist unterfinanziert und wird
meist nur als optionales „Add-on“ verstanden. Um die Situation zu verbessern,
hat die DDG das neue Zertifizierungsmodul „Diabetes und Psyche“
eingeführt.
Das
Modul richtet sich an ambulante und stationäre Diabeteseinrichtungen, die eine
besondere Expertise in der Behandlung von mit Diabetes assoziierten
psychischen Problemen oder diabetes-bezogenen Belastungen nachweisen
können. Das Angebot soll die Transparenz für Patient*innen und Zuweiser*innen
erhöhen und die Qualität der Diabetestherapie in allen Sektoren steigern.
Jeder
dritte Mensch mit Diabetes weist erhöhte diabetesbezogene Belastungen und jeder
achte eine komorbide Depression auf. Aber auch Angst- und Essstörungen
sowie Abhängigkeitserkrankungen und Motivationsprobleme sind bei
Typ-1- und Typ-2-Diabetes weit verbreitet. „Werden diese nicht frühzeitig
fachgerecht identifiziert und behandelt, kann es zu einer Chronifizierung und
schlimmstenfalls lange andauernder Arbeitsunfähigkeit führen.
Das hat neben dem persönlichen Leid auch hohe Kosten für das Gesundheitssystem
zur Folge“, so Professor Dr. Bernhard Kulzer. Er ist Mitglied des Ausschusses
Qualitätssicherung, Schulung und Weiterbildung (QSW) der DDG und Vorsitzender
der AG Diabetes und Psychologie der DDG. Frühzeitige Unterstützung,
Intervention und Beratung können Menschen mit Diabetes helfen.
Zertifikat macht
Expertise der Einrichtung für alle sichtbar
Um
die Versorgung zu verbessern, hat der Ausschuss QSW in Zusammenarbeit mit der
Arbeitsgemeinschaft Diabetes & Psychologie das neue
Zertifizierungsmodul „Diabetes & Psyche“ initiiert. „Das
Zertifikat soll sowohl Menschen mit Diabetes als auch Behandler*innen
transparent machen, welche Einrichtungen eine besondere Expertise in
der psychologischen Behandlungbei Diabetes aufweisen, sodass sie sich
gezielt an sie wenden können“, führt Prof. Kulzer aus.
Das
Zertifikat können ambulante sowie stationäre Behandlungseinrichtungen im Rahmen
der Anerkennungsverfahren „Diabetes Exzellenzzentrum DDG“ und „Diabeteszentrum
DDG“ optional erwerben. Voraussetzung für den Erwerb ist, dass in der
jeweiligen Einrichtung nachgewiesenermaßen ausreichend
Hintergrundwissen über die besonderen Herausforderungen und Probleme von
Menschen mit Diabetes vorliegen. Die Einrichtungen müssen dabei eine definierte
Struktur-, Prozess- und Ergebnisqualität bei der Therapie von Menschen mit
diabetesbezogenen psychischen Belastungen nachweisen. Zertifizierte
Einrichtungen müssen ihre Ergebnisqualität nach einem Zeitraum von
sechs Monaten offenlegen. Durch gezielte Hospitationen und Kooperationen
soll eine verstärkte Vernetzung der zertifizierten Einrichtungen erfolgen, was
die Qualität der Einrichtungen verbessern soll.
„Diese
Maßnahme ist ein wichtiger Schritt, die bisher noch suboptimale psychologische
Betreuung von Menschen mit Diabetes zu verbessern“, erklärt Professor Dr.
rer. nat. Dipl.-Psych. Karin Lange, ehemalige Leiterin der Forschungs- und
Lehreinheit Medizinische Psychologie an der MH Hannover. „Das Zusatzmodul soll
außerdem zeigen, dass psychologische Versorgungsangebote nicht nur ein
‚Nice to have’ bei psychiatrischen Diagnosen sind, sondern – wie in
Leitlinien und DMP gefordert – ein integraler Bestandteil der
Diabetesbehandlung in allen Sektoren sein sollten.
Quelle: Medical Tribune 18.12.2023, Diabetes Letter
10.01.2024
Resolution zur Abbildung von psychosozialen, psychotherapeutischen Leistungen im Krankenhausreformgesetz
„Diabetes und
Psychologie“ ist Gründungsmitglied der Bundesarbeitsgemeinschaft Psychosoziale
Versorgung im Akutkrankenhaus (BAG-PVA), die sich dafür einsetzt, dass psychosoziale und psychotherapeutische
Tätigkeiten im Krankenhaus im Leistungskatalog adäquat abgebildet werden. In
einer aktuellen Resolution der BAG-PAV nimmt diese zu der geplanten Reform der
stationären Behandlung (Krankenhausreformgesetz) und das am 10. Juli 2023 vom
Bundesministerium für Gesundheit (BMG) veröffentlichte Eckpunktepapier zum Krankenhausreformgesetz
Stellung. „Diabetes und Psychologie“ unterstützt diese Stellungnahme und dankt
unserem Mitglied Klaus-Martin Rölver für sein jahrelanges Engagement als
Vertreter von „Diabetes und Psychologie“ in der BAG-PVA.
Hier können Sie die
Stellungnahme im Wortlaut lesen:
Resolution der
Bundesarbeitsgemeinschaft PsychosozialeVersorgung im Akutkrankenhaus (BAG-PVA)
Für die Abbildung
der psychosozialen, neuropsychologischen, psychotherapeutischen und
künstlerischen Therapien in den Vorhaltebudgets und Leistungsgruppen nach dem
Krankenhausreformgesetz
Wir setzen uns dafür ein, dass die notwendigen
Ökonomisierungsprozesse im
Gesundheitswesen nicht zu Lasten einer
notwendigen und effektiven psychosozialen Unterstützung für Patient*innen
erfolgen darf und sich die medizinische Versorgung an den individuellen
Patient*innenbedürfnissen zu orientieren hat.
Die immer komplexer werdende,
hochtechnisierte und -strukturierte medizinische Versorgung in unseren
Krankenhäusern ist für immer mehr und schwerst erkrankte Menschen ohne eine
umfassende psychosoziale Begleitung und Behandlung nicht mehr zeitgemäß.
Daher
fordern wir mit unserer Reaktion auf das am 10. Juli 2023 vom Bundesministerium
für Gesundheit (BMG) veröffentlichte Eckpunktepapier zum
Krankenhausreformgesetz die Abbildung und Integration der OPS-Codierungen der
psychosozialen, neuropsychologischen, psychotherapeutischen und künstlerischen
Therapien in den Leistungsgruppen sowie deren Vorhaltung in den aufgrund von
Schließungen oder Fusionen aufnehmenden Standorten im erforderlichen Umfang.
Für jedes Akutrankenhaus müssen seinen Leistungsbereichen entsprechend nicht
nur spezifisch qualifizierte Fachkräfte wie psychologische und ärztliche
Psychotherapeut*innen bzw. Kinder- und Jugendlichenpsychotherapeut*innen,
Künstlerische Therapeut*innen, Psycholog*innen, Pädagog*innen und
Sozialarbeiter*innen / Sozialpädog*innen zur Verfügung stehen. Sondern es
braucht besonders auch die Verankerung von Fachpsycholog*innen (z. B.
Neuropsycholog*innen, Palliative Care, Psychodiabetolog*:innen,
Psychoonkolog*innen, Intensiv- und Notfallpsycholog*:innen), die gemäß den
Anforderungen nationaler und internationaler Leitlinien eine frühzeitig
einsetzende Behandlung, Unterstützung und Beratung anbieten. Diese Stellen
müssen langfristig angelegt, fest integriert und sicher finanziert sein.
Schwere und chronische körperliche Erkrankungen sind regelhaft mit hohen
psychischen Belastungen verbunden. Werden diese nicht frühzeitig fachgerecht
identifiziert, können diese z. B. durch vermeidbare Folgeerkrankungen,
Chronifizierungen oder lange andauernde Arbeitsunfähigkeit zu hohen Folgekosten
für das Gesundheitssystem führen. Frühzeitige Unterstützung, Intervention und
Beratung fördert den Genesungsprozess und befähigt die betreffenden
Patient*innen und neue Bewältigungsstrategien zu entwickeln.
Zum 1. Juli 2023 hat der Ausschuss Qualität, Schulung und
Weiterbildung (QSW) der DDG die Zusatzmodule „Diabetes & Psyche“ und
„Diabetes & Schwangerschaft“ auf den Weg gebracht. Diese können im Rahmen
der Anerkennungsverfahren zum „Diabetes Exzellenzzentrum DDG“ und
„Diabeteszentrum DDG“ optional erworben werden. Dies ist ein wichtiger Schritt
hin zu einer besseren Sichtbarkeit von psychodiabetologischen Angeboten und
auch ein bedeutsamer Schritt hin zu einer besseren Versorgung. Die Kriterien zum
Erwerb des Zusatzmoduls und die entsprechenden Items zur Struktur-, Prozess-
und Ergebnisqualität finden Sie hier:
Von unseren Mitgliedern Rainer Paust, Renate Rita
Krämer-Paust, Uwe Schönrade und Bianca Thoma ist ganz aktuell das Buch
„Praxisbuch Psychodiabetologie. Psychosoziale Aspekte der Diabetes-Behandlung“
im Deutschen Ärzteverlag (2023, 267 Seiten + XVIII Vorspann, 28 Abbildungen und
38 Tabellen) als gedrucktes Buch und e-Book erschienen.
Die Autoren schreiben: „Für eine personenzentrierte Beratung hilft es Ihnen,
individuelle psychosoziale Faktoren und daraus resultierende
Behandlungsbarrieren zu erkennen, um daraus entsprechende therapierelevante
Ableitungen zu treffen. Neben theoretischen Bausteinen stehen in diesem Werk
praktische Anwendungsbeispiele mit Gesprächs- und Fragetechniken im Fokus.
Zahlreiche Fallbeispiele aus der Praxis verdeutlichen Ihnen, wie eine
personenzentrierte Beratung unter Alltagsbedingungen angewendet werden kann“.
Unser Fazit: Sehr empfehlenswert!
Hohe Auszeichnungen für Prof. Dr. Karin Lange (Hannover)
Auf der diesjährigen Mitgliederversammlung der AG Diabetes und Psychologie des Vereins Diabetes und Psychologie wurde Frau Dr. Karin Lange als 1. Ehrenmitglied ausgezeichnet.
Verleihung der Ehrenmitgliedschaft
Verleihung der DDG-Ehrennadel in Gold
Frau Prof. Lange war Gründungsmitglied des Vereins und engagierte sich jahrzehntelang im Vorstand des Vereins und als Verantwortliche für die Weiterbildung zum Fachpsychologen Diabetes bzw. die spezielle Psychotherapie Diabetes. Auf der Tagung der DDG 2023 in Berlin wurde ihr zudem als erste Frau die DDG-Ehrennadel verliehen. Damit werden Mitglieder der Deutschen Diabetes Gesellschaft geehrt, die sich im besonderen Maße für die deutsche und internationale Diabetologie engagiert haben. In einer kurzen Rede würdigte Prof. Kulzer als Laudator bei der Verleihung des Preises das wissenschaftliche Wirken von Frau Prof. Lange und ihre Verdienste für die deutsche Diabetologie im Allgemeinen, aber besonders auch ihr Engagement für die Psychodiabetologie. Neben der Urkunde der DDG durfte er auch das Präsent des Vereins, ein Unikat übereichen. Vielen Dank Karin für dein herausragendes Engagement!
Dr. Andrea Benecke zur Präsidentin der Bundespsychotherapeutenkammer gewählt
Das neu gewählte Vorstand der Bundespsychotherapeutenkammer:
Von links nach rechts: Cornelia Metge, Nikolaus Melcop, Andrea Benecke, Sabine Maur und Wolfgang Schreck /BPtK, Raman El Atiaoui
Auf dem 42. Deutsche Psychotherapeutentag wurde mit Dr. Andrea Benecke erstmals in der 20-jährigen Geschichte der Kammer eine Frau als Präsidentin gewählt. Die Bundespsychotherapeutenkammer vertritt die Interessen der ca. 59.000 niedergelassenen und angestellten Psychologischen Psychotherapeutinnen und -therapeuten und Kinder- und Jugendlichenpsychotherapeutinnen und -therapeuten in Deutschland. Frau Benecke ist seit langem engagiertes Mitglied im Verein Diabetes und Psychologie und hat unter anderem in Mainz die Spezialambulanz Psychodiabetologie aufgebaut. Wir gratulieren Frau Benecke ganz herzlich zu ihrer Wahl und freuen uns mit ihr. Du machst das sicher sehr gut, Andrea!
Nachruf auf Dr. Axel Hirsch
Im Alter von 79 Jahren ist Dr. Axel Hirsch (13.11.1942 – 21.11.2021), ein Pionier moderner Therapie- und Schulungskonzepte und Fürsprecher für die Rechte von Menschen mit Diabetes gestorben. Während seiner Zeit als Assistent am psychologischen Lehrstuhl in Hamburg ist Axel Hirsch an Typ-1-Diabetes erkrankt. Dies weckte in ihm die Neugier, mehr über psychologische Konzepte des Diabetes zu erfahren und auf diesem Gebiet zu forschen. Auf seine Initiative hin ist es maßgeblich zurückzuführen, dass sich 1985 erstmals eine kleine Gruppe von Psychologen traf, um sich über psychologische Konzepte des Diabetes auszutauschen, woraus 1986 der "Arbeitskreis Diabetes und Psychologie" entstand. 1990 wurde dieser dann in den gemeinnützigen Verein „Diabetes und Psychologie e.V.“ umgewandelt, seit 1992 auch als offizielle Arbeitsgemeinschaft der Deutschen Diabetes Gesellschaft (DDG). Axel Hirsch war die treibende Kraft hinter dieser Initiative und bis 1989 1. Vorsitzender. Auch auf europäischer Ebene suchte er den Austausch mit Kollegen und war ebenfalls 1998 Gründungs- und Vorstandsmitglied der Studiengruppe PSAD – (Psychosocial Aspects of Diabetes Study Group) der europäischen Diabetes-Gesellschaft (EASD). Als klinischer Psychologe am Krankenhaus Bethanien (Hamburg) war Axel Hirsch einer der ersten Psychologen, der kontinuierlich im Diabetes-Team arbeitete.
Mit Axel Hirsch ist vor allem der Begriff „Empowerment“ verbunden – dem Anliegen, dass Menschen mit Diabetes ihr Leben und auch ihre Diabetestherapie selbstständig nach eigenen Zielen, Werten und Überzeugungen gestalten. Gemeint ist damit, dass nicht Ärzte oder andere Experten über die Therapie entscheiden, sondern Menschen mit Diabetes diese selbst für sich bestimmen. Was mittlerweile Standard und auch in den aktuellen Leitlinien, dem Patientenrechtegesetz so zu finden ist, war zu der damaligen Zeit keine Selbstverständlichkeit. Um Patienten zu stärken, schrieb er eines der ersten Patientenbücher zum Typ-1-Diabetes, welches auch heute noch als Neuauflage verfügbar ist, sein Buch mit dem programmatischen Titel „Diabetes ist meine Sache“ ist ebenfalls noch beim Kirchheim-Verlag erhältlich. Als Autor schrieb er regemäßig über psychologische Themen des Diabetes, veröffentlichte zahlreiche Publikationen und war ein gefragter Redner auf Kongressen und in der Fort- und Weitebildung. Nach seiner Pensionierung zog er mit seiner Frau nach Spanien, von wo er aus viele Reisen machte und sich leidenschaftlich der Botanik widmete.
Ohne Zweifel kann Axel Hirsch als ein Visionär bezeichnet werden, der mit seiner fortschrittlichen und kritischen Denkweise viele Impulse in der Diabetologie gesetzt hat, die noch heute spür- und greifbarbar sind. Danke Axel, was du für Menschen mit Diabetes und unseren Verein „Diabetes und Psychologie“ geleistet hast, danke für viele prägende Erlebnisse mit dir.
Prof. Dr. Bernhard Kulzer (Bad Mergentheim)
Neues Konsenspapier der Amerikanische Diabetes Association (ADA) und
der Europäischen Diabetes-Gesellschaft (EASD) zum Typ-1-Diabetes
Psychosoziale Belastungen rücken stärker in den Mittelpunkt
Besonderes Augenmerk legt der aktuelle Report diesmal auf den Umgang mit psychosozialen Belastungen
im Zusammenhang mit Typ-1-Diabetes. So wird in dem Report berichtet,
dass ca. 20–40% aller Menschen mit Typ-1-Diabetes erhöhten
diabetesassoziierten emotionalen Stress aufweisen, der sich negativ auf
Krankheitsbewältigung und Selbstmanagement auswirkt. Zudem treten
Depressionen häufiger als in der allgemeinen Bevölkerung auf – ca. 15%
der Menschen mit Typ-1-Diabetes sind davon betroffen.
Auch die Bedeutung der strukturierten Diabetesschulungen
wird hervorgehoben, in denen Menschen mit Diabetes einerseits das
erforderliche grundlegende Wissen und therapierelevante Fertigkeiten
erwerben können, aber auch den Umgang mit psychosozialen Belastungen
erlernen.
Psychische Probleme sind neben Faktoren wie niedrigem
sozioökonomischem Status, hohen HbA1c-Werten, mangelnden Fähigkeiten zum
Selbstmanagement, somatischen Begleiterkrankungen, Infektionen,
Alkohol- und Drogenmissbrauch auch Risikofaktoren für das Auftreten von
Akutkomplikationen wie diabetische Ketoazidosen und Hypoglykämien.
Holt, R.I.G., DeVries, J.H., Hess-Fischl, A. et
al. The management of type 1 diabetes in adults. A consensus report by
the American Diabetes Association (ADA) and the European Association for
the Study of Diabetes (EASD). Diabetologia 64, 2609–2652 (2021). https://doi.org/10.1007/s00125-021-05568-3
Pressemitteilung
Depressionen, Angst, Essstörungen: DDG
und DAG warnen vor unzureichender psychischer Versorgung von Menschen
mit Diabetes und Übergewicht
Wie gut Menschen mit Diabetes oder Adipositas mit ihrer
Erkrankung leben können, hängt nicht zuletzt davon ab, wie zuverlässig
sie die notwendige Selbstbehandlung – vom Blutzuckermessen über Bewegung
bis hin zu einer angepassten Ernährung – meistern. Denn psychische
Erkrankungen wie Depressionen und Ess- oder Angststörungen behindern die
Selbstmanagementfähigkeiten immens. Dennoch fehlt es derzeit an
ausreichend ausgebildeten Psychotherapeutinnen und -therapeuten,
ambulanten Beratungsstellen und niederschwelliger Unterstützung. Wie die
psychosoziale Versorgung Betroffener verbessert werden kann, erläutern
Expertinnen und Experten der Deutschen Diabetes Gesellschaft (DDG) und
der Deutschen Adipositas-Gesellschaft (DAG) bei einer Pressekonferenz am
5. November 2021, die anlässlich der Diabetes Herbsttagung in Wiesbaden
sowie online stattfindet.
Nationale VersorgungsLeitlinie (NVL) Typ-2-Diabetes
(NVL Typ-2-Diabetes, Teilpublikation der Langfassung – 2. Auflage, Version 1, 2021, S. 20)
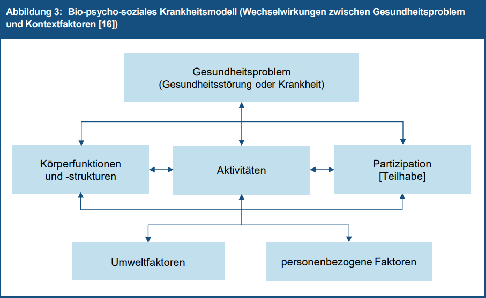
Mitglieder des Vereins haben aktiv an der „Nationale VersorgungsLeitlinie (NVL) Typ-2-Diabetes“ mitgearbeitet. Die ersten beiden Kapitel (Medikamentöse Therapie des Glukosestoffwechsels und Partizipative Entscheidungsfindung) sind hier veröffentlicht. In dem ersten Kapitel „Partizipative Entscheidungsfindung“ wird auf die Notwendigkeit des Einbezugs des Patienten in alle Entscheidungsprozesse und die Anwendung eines biopsychosozialen Krankheitsmodells verwiesen.
Spezielle Psychotherapie Diabetes jetzt
auch in Baden-Württemberg
Am
20.10.2018 hat die Vertreterversammlung der Psychotherapeutenkammer
Baden-Württemberg, mehrheitlich beschlossen, die Weiterbildungsordnung um die
„Spezielle Psychotherapie Diabetes“ zu ergänzen.
Damit ist die
Psychotherapeutenkammer Baden-Württemberg nach Rheinland-Pfalz und Bayern die
3. Kammer, die die Empfehlungen der Bundespsychotherapeutenkammer nach einer
speziellen Weiterbildung auf Länderebene umsetzt.
„Common Toolbox“
Eine Auswahl von diabetesrelevanten psychometrischen Fragebögen für die Forschung und Praxis.
Zur Wissenschaftlichen Tagung der Arbeitsgruppe "Mental Aspects of Diabetes" des Kompetenznetzes Diabetes am 25. September 2015.
Thema: "Psychische Aspekte des Diabetes: Harmonisierung psychometrischer Messinstrumente
„Diabetes und Psychologie e.V.“ ist seit Jahren Mitglied der „Bundesarbeitsgemeinschaft psychosoziale Versorgung im Akutkrankenhaus“, die sich für eine angemessene Honorierung psychologischer/psychotherapeutischer Leistungen im Akutkrankenhaus einsetzt. Als eine Maßnahme wird seitens der BAG-PVA die Verbesserung der Kodierung psychosozialer Interventionen im OPS (Operationen- und Prozeduren-Schlüssel) angestrebt.
Anbei finden Sie hier den aktualisierten Kodierleitfaden 2015, der dazu beitragen soll, dass psychosoziale Interventionen im Bereich Diabetes und anderen Erkrankungen möglichst umfassend und richtig kodiert werden.
Erweiterung des Curriculums Fachpsychologe vom Vorstand der DDG (Vorstandssitzung vom 20.11.2014) genehmigt
Im Rahmen der Ausbildung zum Fachpsychologen/in Diabetes DDG
und zum Psychodiabetologen/in wird ab 2105 ein zusätzliches Seminar
„Verhaltensmedizinische Grundlagen des Diabetes bei Kinder und Jugendlichen“ angeboten. Das neu entwickelte
Seminarangebot richtet sich an Psychologen/innen, Kinder- und
Jugendpsychotherapeuten sowie andere in der Beratung Kindern mit Diabetes tätige
Teammitglieder. Die Teilnehmer/innen erhalten zunächst komprimierte
Informationen über den aktuellen Stand der pädiatrischen Diabetologie und über
die psychosoziale Situation betroffener Familie. Daran anschließend erarbeiten
sie Beratungsangebote und Interventionen, die sie als Mitglieder eines
multiprofessionellen pädiatrischen Diabetesteams in die Lage versetzen, diese
in der Patienten-schulung, psychosozialen Beratung und ggf. auch
psychotherapeutisch einzusetzen.
Im Seminar werden:
die Grundlagen einer modernen Diabetestherapie
mit einer Insulinpumpe und CGM bei Kindern und Jugendlichen theoretisch und
praktisch vermittelt;
altersgemäße Therapieziele entsprechend der
aktuellen evidenzbasierten Leitlinien erarbeitet;
aktuelle entwicklungspsychologische Grundlagen
bezogen auf den Diabetes reflektiert:
diabetesspezifische psychosoziale Belastungen
und Ängste von Eltern und Kindern in verschiedenen Lebens- und Diabetesphasen
am Beispiel von Kasuistiken dargestellt und Hilfsangebote erarbeitet;
die gesetzlichen Grundlagen für psychosoziale
Hilfen dargestellt;
Konzepte für psychosoziale Beratungen im Kontext
der Diabetesschulungen stationär und ambulant sowie während der ambulanten
Langzeitbetreuung dargestellt und einzelne Sequenzen praktisch trainiert;
die Prävalenz und Ausprägung von psychischen
Störungen bei Kindern und Jugendlichen mit Diabetes sowie ihren Eltern
vorgestellt;
diabetesspezifische psychotherapeutische
Konzepte, z. B. bei Hypoglykämieangst, Non-Adhärenz oder Depression /
Resignation bei Jugendlichen, Essstörungen mit Insulinpurging, dargestellt und
praktisch erarbeitet.
kinder- und jugendspezifische psychologische
Messinstrumente und Fragebogen vorgestellt;
Möglichkeiten der Kooperation und Delegation
(Kinder- und Jugendpsychiatrie, Rehabilitation, Jugendamt) aufgezeigt.
Für Kolleginnen und Kollegen, die ausschließlich in der
Versorgung von Kindern und Jugendlichen mit Diabetes tätig sind, ersetzt dieses
Seminar das Seminar „Verhaltensmedizinische Grundlagen des Diabetes 2“, in dem
der Typ-2-Diabetes im Erwachsenenalter bearbeitet wird.
Lesen Sie hier den vollständigen Text (Hintergrund, Literatur)
„Neue S2-Leitlinie Psychosoziales und Diabetes"
Dr. Erhard Siegel, Präsident der
Deutschen Diabetes Gesellschaft (l.)
und PD Dr. Bernhard Kulzer (r.)
Diabetes Zentrum Mergentheim
auf der Pressekonferenz in Berlin.
Um die Behandlung von Diabetespatienten zu verbessern, hat die Deutsche Diabetes Gesellschaft (DDG) unter Federführung von Dr. Bernhard Kulzer vom Diabetes Zentrum Mergentheim in Berlin im Haus der Bundespressekonferenz die weltweit erste Leitlinie zum Thema „Psychosoziales und Diabetes“ vorgestellt.
Auf großes Medienecho stieß die Vorstellung der Leitlinie, an der sieben führende Experten aus der Diabetologie, Psychosomatik, Psychologie und Psychiatrie fachübergreifend zusammengearbeitet haben.